Article
Outrunning Cancer-Related Fatigue
Author(s):
People who have had cancer often contend with deep, pervasive exhaustion. The counterintuitive cure: exercise.
When Honora Miller, 53, wondered how to explain her cancer-related fatigue to her son, a friend recommended using an analogy involving spoons. The spoon theory held that Miller would start each day with a certain number of the utensils, each one representing energy. Each daily activity cost a spoon.
“Let’s say I only have 10 spoons today, but I do more than I should, in a sense borrowing from tomorrow’s spoons. I know that tomorrow will have to be a rest day because I won’t have enough spoons,” Miller says she told her son. “It has become a shorthand for us. My 14-year-old understands that is why some days after I pick him up I have to go home and go to sleep.”
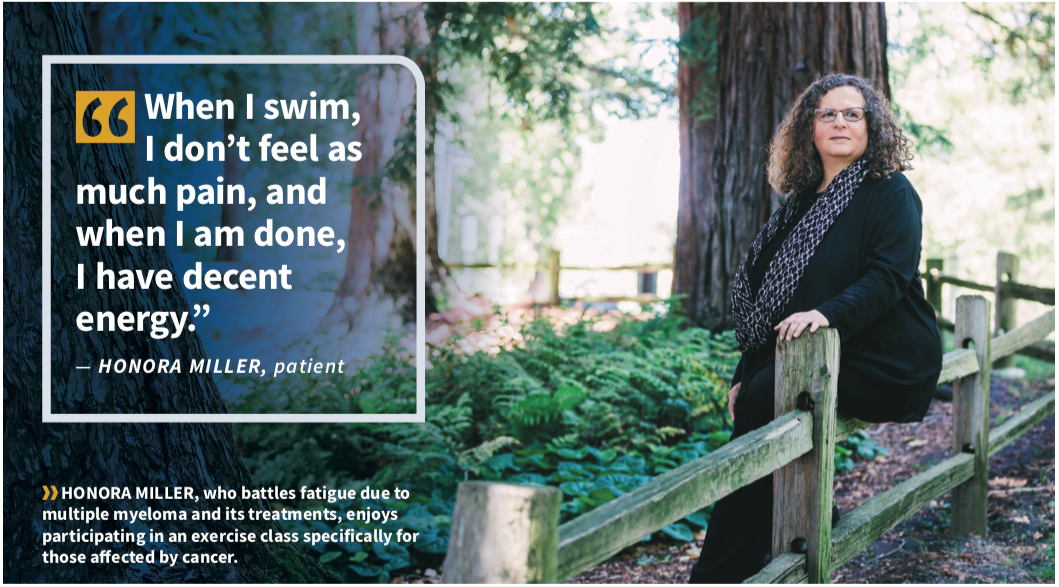
Miller has multiple myeloma, a cancer involving malignant plasma cells that grow abnormally in bone marrow, and has had to adapt to the day-to-day management of fatigue that accompanies the disease and its treatments. Cancer-related fatigue can be defined as a distressing, persistent sense of physical, emotional and/or mental tiredness or exhaustion related to cancer and/or its treatment that is out of proportion to recent activity and interferes with usual function. People with all kinds of cancer report this common side effect, and many surveys of patients with advanced cancer rank fatigue as the most disturbing symptom.
“Unlike other forms of fatigue or tiredness, cancer-related fatigue is not relieved by your typical rest,” says Dr. Carmen Escalante, professor and chair of the department of general internal medicine at The University of Texas MD Anderson Cancer Center in Houston. “These people do not wake up feeling refreshed after a good night’s sleep.”
Between 80% and 100% of people with cancer report experiencing fatigue, and sometimes the symptoms extend years into survivorship.


Experts such as Escalante do not yet know the exact cause or why certain patients experience more cancer-related fatigue than others. “There are a lot of factors to consider when evaluating for fatigue, including the cancer’s stage, the extent of the disease, and past and current treatments,” Escalante says. “Patients with more extensive disease and those who have undergone multimodality treatments, like combinations of chemotherapy, radiation, hormonal therapy and surgical treatments, do seem to have more cancer-related fatigue.”
Some study findings suggest that the number of markers in the blood that indicate inflammation, such as C-reactive protein or certain fatty acids, could also increase the risk of cancer-related fatigue.
PINPOINTING THE CAUSE
Miller experienced debilitating fatigue before she knew she had cancer. She recalls taking her son to a museum and napping on a bench while he looked around; before that, she’d had enough energy to hike and bike for miles. Her inability to do what she normally could prompted her persistence to find out what was behind the fatigue. After receiving her diagnosis and starting treatment for myeloma, Miller discussed her fatigue with her specialists. Outside of clinical trials, doctors do not always administer specific questionnaires to diagnose cancer-related fatigue.
“Often, we start by looking at fatigue as a subjective experience,” says Leigh Kinczewski, a certified registered nurse practitioner in the supportive oncology and palliative care program at Fox Chase Cancer Center in Philadelphia. “It is something that is emotional, cognitive and germane to how the patient is feeling and is not well captured with bloodwork, imaging and other objective measures.”
In some cases, Kinczewski says, a simple numeric scale is used. “I may ask the patient to think back over their last seven days to capture how they have been feeling recently,” she says. “A response of 0-3 is mild fatigue; 4-6, moderate fatigue; and 7-10, severe fatigue.” Patients with moderate to severe fatigue may be asked follow-up questions to identify patterns or assess its duration.
Miller also underwent a thorough assessment with a palliative care team to determine if other factors were contributing to her fatigue. Cancer-related fatigue rarely occurs on its own and is often diagnosed along with symptoms such as pain, depression, anxiety, anemia and sleep disturbances.
“The consensus, almost without exception, is that depression is consistently associated with fatigue at an at least moderate level, but it is unclear whether being fatigued causes people to be depressed, if the depression is causing the fatigue or if they are occurring in different pathways,” Kinczewski says.
Treating the depression can sometimes lower the level of fatigue, Escalante says.
A thorough general medical history and review of recent treatments and medications can also reveal other sources of fatigue. For example, patients with under- lying conditions such as heart failure, past coronary disease, diabetes, kidney disease, thyroid disorders and anemia may experience fatigue.
“Many of our patients with cancer are 50 or older,” Escalante says. “Often, trying to understand the status of those other comorbidities can be helpful in deter- mining whether they are contributing to the overall level of fatigue.”


Fatigue can also stem from treatment for these conditions, with medications such as beta blockers, opioids, antidepressants, nausea drugs and some antihistamines, Kinczewski adds. “Oftentimes, if I have a patient with fatigue, I will look at their medication list and discuss with them and their providers alternative medications or dose reductions,” she says.
In Miller’s case, her health care team opted to manage her pain before addressing her fatigue. Prior to undergoing a stem cell transplant, a procedure that replaces damaged stem cells with healthy ones, Miller had received very high doses of a chemotherapy drug called melphalan. As a result, she dealt with significant joint pain. “It was really when we managed the pain that I was able to turn my attention to managing my fatigue,” Miller says.
CHOOSING A TREATMENT
For Charles Tucker, 60, cancer-related fatigue came on gradually as he got deeper into treatment. Like Miller, Tucker has multiple myeloma.
Prior to his 2016 diagnosis, Tucker was an active power walker, runner and long-distance cyclist. Once he began radiation therapy and then chemotherapy, he began to feel as though he was in a fog. “It is hard to describe, but every day, I was taking breaks and taking naps. I was lying down more,” Tucker recalls. “You feel like your body shouldn’t be moving, like it can’t move.”
The only thing that helped, he says, was to do the opposite of what his body told him to do. He got moving.
The many recommended or tested treatments for cancer-related fatigue mostly fall under two categories: pharmaceutical and nonpharmaceutical.
“For pharmaceutical options, there are two primary options we consider: corticosteroids and Ritalin (meth- ylphenidate),” Kinczewski says. “Corticosteroids can work well in certain circumstances but cause side effects such as increased blood pressure or muscle weakness, so we often only use them in short-term situations and for patients who are rather ill.”
Ritalin is a stimulant and classified as a psychotropic drug, as is another medication approved for narcolepsy, Provigil (modafinil). Whereas some evidence backs Ritalin’s effectiveness in alleviating cancer-related fatigue, the data supporting Provigil are less clear-cut.
“The National Comprehensive Cancer Network recommends using Ritalin cautiously,” Kinczewski says. “Provigil and other drugs like antidepressants are not recommended when the primary indication is cancer-related fatigue.”
Nonpharmaceutical options may bring more success. Findings from a study comparing types of treatment for cancer-related fatigue showed that psychological interventions, such as cognitive behavioral and psycho- educational therapy, and exercise improved symptoms but drugs did not.
“The research that has been done, especially in breast cancer but in other cancers too, has been consistent in showing that resistance training together with aerobic exercise is a very worthwhile strategy against cancer- related fatigue,” says Cornelia Ulrich, executive director of the Comprehensive Cancer Center at the University of Utah’s Huntsman Cancer Institute in Salt Lake City.
The frequency, amount and type of exercise vary by study, but everyone agrees that any exercise is better than nothing. “We know that exercise helps,” Escalante says.
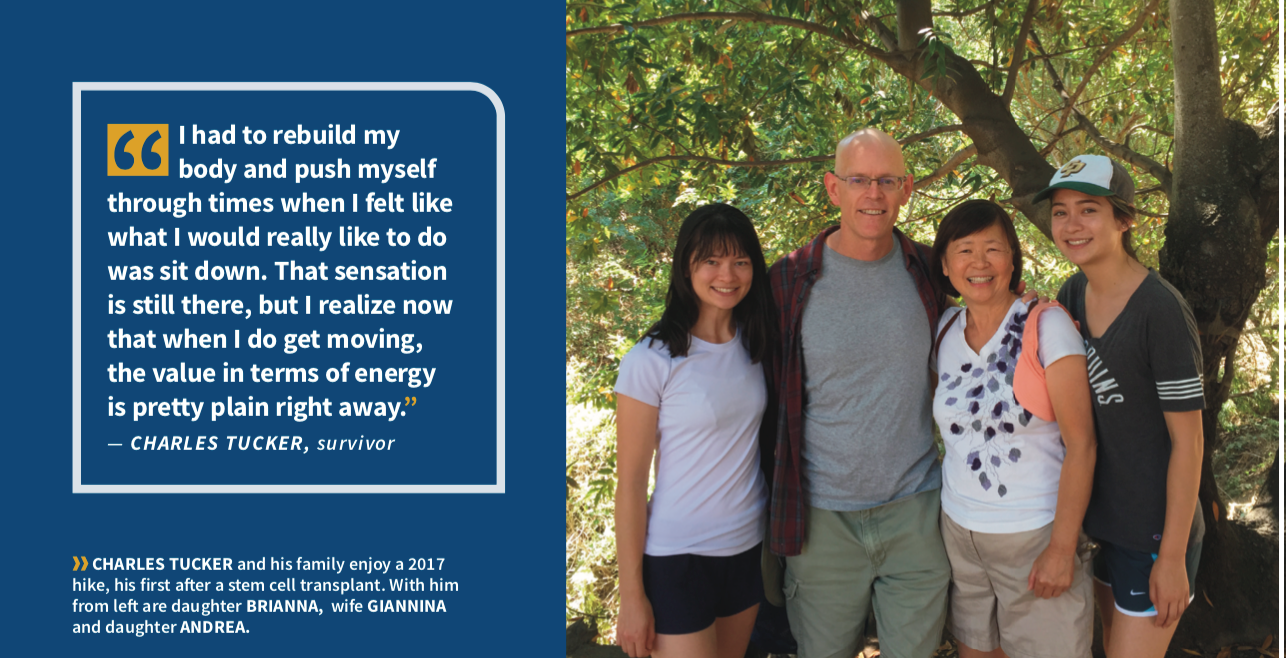
After eventually undergoing a stem cell transplant, Tucker actively retrained his body. Initially, exercise meant a lap around the hospital ward. Weeks and months later, he was power walking four to five miles.
“I had to rebuild my body and push myself through times when I felt like what I would really like to do was sit down,” Tucker says. “That sensation is still there, but I realize now that when I do get moving, the value in terms of energy is pretty plain right away.”
Miller agrees that the payoff is almost immediate. “In particular, when I swim, I don’t feel as much pain, and when I am done, I have decent energy,” she says. “I may still have to nap later, but in the time around the swim, I have a boost of energy for the next couple of days.” When she takes a break from regular exercise, her energy declines, she says.
Although there are no specific recommendations regarding the amount of activity, many studies looking into the effects of exercise had participants engage in physical activity about three times a week, Ulrich says.
“What is encouraging, as well, is that the effect seems to be consistent across multiple types of cancer, whether it is breast, pancreatic or prostate,” she says. “Although this fatigue cannot exactly be prevented, what is critical is that these exercise regimens be implemented at the time when patients are experiencing the most fatigue.”
Miller has also tried several pharmacologic solutions. Provigil, she says, gave her the jitters and no energy. She also recently tried Vyvanse (lisdexamfetamine dimesylate), a stimulant for attention-deficit/hyperactivity disorder; it boosted her energy but also kept her awake at night.
“Exercise is what works best for me, but I have also spoken to others where Provigil is the thing that works for them, or Adderall (dextroamphetamine plus amphetamine),” she says. “Different people have different paths.”
A wide variety of other methods to relieve fatigue have been tested in clinical trials with moderate success. These approaches include yoga, massage, acupuncture and acupressure aimed at relaxation rather than stimulation, but Kinczewski notes that these methods are not accessible or appropriate for every patient.
Could diet play a role? Escalante says that there are no effective dietary strategies for cancer-related fatigue, but an individual’s diet can exacerbate symptoms. “If a patient is not eating well or not eating the right foods, I tell them that may be contributing,” she says.
The results of one randomized trial of American ginseng showed improvement, compared with placebo, among fatigued cancer survivors. No benefits have been seen with other supplements, including Coenzyme Q10 and L-carnitine.
Patients regularly have bloodwork done to look for imbalances in nutrients such as sodium, potassium, calcium, iron and magnesium, Kinczewski said. Taking supplements to correct known deficiencies may help patients feel more energetic. However, there is no routinely recommended dietary strategy, she said.
LIVING WITH LOW ENERGY
Miller and Tucker have more than myeloma in common. They both regularly attend Exercise for Energy and Exercise for Strength programs led by Joanna M. Losito, a nurse at Palo Alto Medical Foundation of Sutter Health in Mountain View and Sunnyvale, California.
“I met Joanna at the infusion center where she works, and she encouraged me to attend,” Tucker recalls. “Joanna’s class was so important to my journey because it was led by somebody who understands and specializes in cancer-related fatigue. It was incredibly valuable.”
Having a place to go where you feel understood and supported is very important, Miller agrees. A couple of years into her battle with myeloma, she was forced to leave a demanding but beloved career in social work. Miller choked up as she discussed having to accept that she can no longer work in her profession. “It is an ongoing process, coming to terms with that, with accepting these new realities,” Miller says.
Instead of focusing on that loss, she tries to turn her attention to what she can control. Regular exercise and dietary changes led to a desirable 80-pound weight loss in the last year. She strives to remain as healthy as possible for as long as possible and practices the art of being compassionate toward herself. “That takes a lot of intentionality,” Miller says. “My life looks different now.”
Both Miller and Tucker describe their myeloma as under control but continue to receive maintenance treatments. Additionally, both have been told by their physicians that much of their current fatigue is likely caused by treatments they received over the past few years to keep the disease in check.
“It was profound for me to realize that it was the treatment that was doing this to me and that I could get through it,” Tucker says.
Miller says she didn’t want to assign blame for how she felt but found it reassuring and helpful to understand that tradeoff.
“It is important for patients to hear that this is not just in their head and that it is a true challenge,” Ulrich says. “The biggest message I would give to people facing cancer-related fatigue is that once they get over that initial hump of getting up and getting started even when they don’t feel well, exercise can really make a difference in how they feel.”







